History |
Currently, the gold standard for measuring kidney function through glomerular filtration rate (GFR) uses creatinine, a metabolite of muscle breakdown. In the 1999 Modification of Diet in Renal Disease (MDRD) study, researchers observed Black study participants (n=197) had, on average, higher glomerular filtration rates (GFR) when compared to White participants with the same creatinine level. The researchers assumed that Black participants had higher muscle mass to explain the higher creatinine and GFR levels. Levey et al. then incorporated a race correlation factor as a proxy for the muscle mass in the estimated GFR (eGFR) equation. This clinical segregation is not only exclusive by perpetuates the idea of Black "otherhood" while simultaneously assuming that all other races and ethnicities are equivalent to those of white patients.
Race is a social construct rooted in oppression. The assumption that races are biologically different, as assumed in race-based equations such as MDRD and CDK-EPI reflects a flawed science that results in inequitable health outcomes. These include racial and ethnic disparities seen in lower referrals to nephrologists, longer waiting times for transplantation, and overall lower rates of transplantation in historically minoritized groups. eGFR = 186 × Serum Cr-1.154 × age-0.203 × 1.212 (if Black) × 0.742 (if female)
|
New 2021 Recommendations for Calculating eGFR
The National Kidney Foundation (NKF) and the American Society of Nephrology (ASN) teamed up in the summer of 2020 to create a task force on Reassessing the Inclusion of Race in Diagnosing Kidney Diseases with the aim of standardizing the adoption of a non-race-based eGFR equation allowing for equitable and unbiased care for patients with kidney disease. In the final report, released in September 2021, the task force urges all healthcare systems to adopt a new eGFR 2021 CKD EPI creatinine equation that does not include race. They also recommend institutions to increase the use of cystatin C in addition to serum creatinine to confirm the assessment of kidney function.
What is Cystatin C?
|
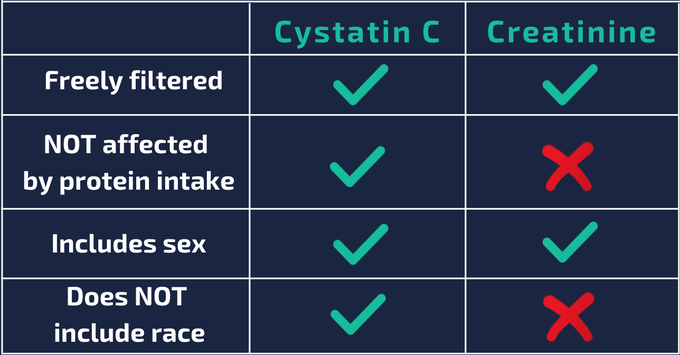
Cystatin C is a low-molecular weight protease inhibitor, produced by all nucleated cells at a constant rate and freely filtered and fully catabolized in the proximal tubule, making it a useful marker of GFR. Cystatin C has also been shown to better predict adverse cardiovascular outcomes and mortality in comparison to creatinine. While creatinine serum concentrations depend on a variety of factors, cystatin C is produced at a constant rate, so its plasma concentration is mainly solely dependent on GFR. |
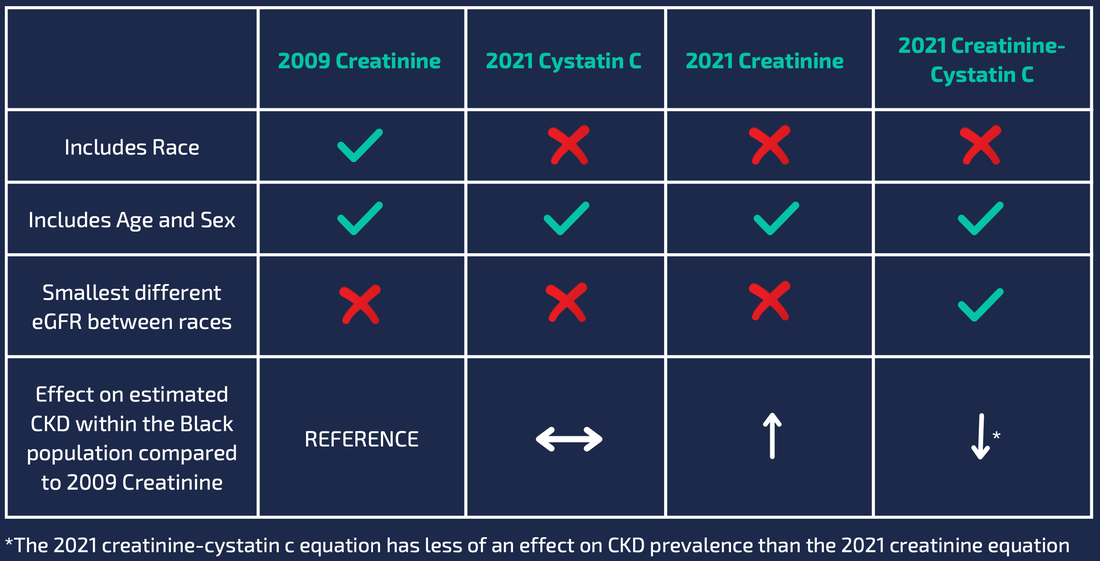
Equation comparison
For use of the new equations, we suggest using the MDCalc website
Toolkit
FliersFliers you can distribute to help spread the word about the significance of the eGFR equation change
|
PowerpointPresent a brief history and importance of not using race-based eGFR to your clinical team! 5 min presentation w/ references ready to go!
Subspecialty specific slides |
ResourcesLooking for an in depth dive into race-base medicine, the original studies that created the eGFR equation, what cystatin C is and newly proposed non-race-based eGFR equations? Find the resource list here!
| ||||||
